Reprinted from N.C. Health News
State health officials, worried about having resources to fight a potential outbreak of the Zika virus in North Carolina, were heartened this month when President Barack Obama asked Congress for $1.8 billion to combat the spread of the potentially debilitating disease.
Supporter Spotlight

Budget cuts have left state and local health departments understaffed and, officials say, in a precariously dangerous situation if the country has to face outbreaks of two or more infectious diseases – such as Zika, new strains of flu or the West Nile and Ebola viruses – at the same time.

“We have been lucky,” said James Blumenstock of the Association of State and Territorial Health Officials of states’ and localities’ ability to contain the flu, West Nile and Ebola threats of the last five years.
“Not only have the last major threats not been as severe as they might have been, they have also been sequential,” Blumenstock said. “The issue is: What if the next pandemic is not as mild as the last ones? What if more than one of them happens at once?”
States to varying degrees have cut back spending on public health since the onset of the Great Recession in 2007. Overall state spending on public health fell by $1.3 billion between 2008 and 2014, two health research organizations – the Trust for America’s Health and the Robert Wood Johnson Foundation – reported last year.
And the trend didn’t end as the economy improved. Sixteen states reduced spending between fiscal 2013 and 2015, the two organizations said in another report. Those were the same years the nation faced Ebola, a new outbreak of West Nile and, in 2014, widespread cases of the H3N2 flu strain.
Supporter Spotlight

States with the biggest cuts over that time: California (13.3 percent), Massachusetts (11.6 percent) and Washington (11.1 percent). Six states – Alabama, Indiana, Kansas, North Carolina, Ohio and Washington – cut their spending all three years.
Local health departments have suffered too. They lost nearly 52,000 staff positions as a result of hiring freezes and budget cuts between 2008 and 2014, the National Association of County and City Health Officials reports.
“The steady reduction in public health funding has resulted in a progressive erosion of manpower and the capacity to do the kind of work that would be optimal,” said Jeff Duchin, chief medical officer in Seattle and King County. “Quite frankly, we just don’t have the staff we need.”
Mosquito monitoring suffers
Health officials are confident they could contain an outbreak of the Zika virus if Congress approves the president’s request for money, which would go to eradicating the mosquitoes that spread it, research into vaccines to inoculate people against it and public education about prevention.
As of last week, the Centers for Disease Control and Prevention reported 92 confirmed cases in the United States, including the U.S. territories. In almost every case, the patients are believed to have been infected by mosquitoes, either abroad or at home in Puerto Rico.
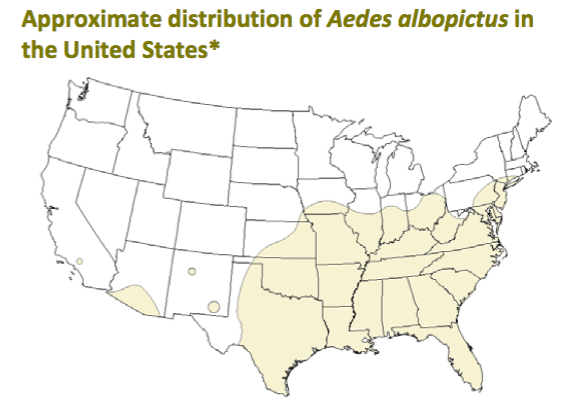
The mosquito that transmits the virus, the Aedes aegypti, breeds in the United States and the rest of the Americas, and is also a carrier of dengue, chikungunya and yellow fever. Scientists say that with international travel and Zika outbreaks in more than two dozen Latin American countries, it is inevitable that mosquitoes carrying Zika will surface here.
Zika poses little threat to most people, but it is potentially very dangerous for pregnant women. There is increasing evidence in Brazil – which had a virulent outbreak of Zika last spring – that the virus causes a birth defect, known as microcephaly, in which children are born with unusually small heads and brains.
That Zika is spread mainly by mosquitoes particularly alarms health officials.
A 2014 report by the Council of State and Territorial Epidemiologists found that state and local health departments are less prepared to track and contain mosquito-borne infections than at any time since the early 2000s, when they ramped up to deal with the first outbreak of another mosquito-borne illness, the West Nile virus.
Between 2004 and 2012, there was a 41 percent drop in the number of staff working at least half time in mosquito surveillance (to detect if they are carrying disease), according to the report. Seven states no longer conduct mosquito surveillance.
Surveillance for mosquito-borne viruses other than West Nile runs from patchy to absent in the states, the report said. “In particular,” it said, “public health laboratory capacity for proactive surveillance is poor to nonexistent in most states.”
Even with West Nile, declining mosquito surveillance contributed to a new spike in cases in 2012, particularly in the Dallas area, said Jeff Engel, director of the Council of State and Territorial Epidemiologists. “We let our guard down.”
More than mosquito surveillance has suffered in the budget cuts. The Association of State and Territorial Health Officials reports that since 2008, 20 state health agencies have cut programs for sexually transmitted diseases, including AIDS, and 15 have cut laboratory services.
“Funding has been reduced for public health activities at the same time that public health threats are coming more often and more vigorously and with more intensity,” Blumenstock said.
Redeploying staff
When a new infectious disease such as Zika emerges, state and local health departments face a multitude of tasks: isolating and containing the threat, identifying people who are infected and assuring they are treated, reporting cases to the CDC, coordinating responses with hospitals and other agencies, performing necessary laboratory work and educating the public and the medical community.
To cope with an infectious-disease outbreak amid reduced budgets, state and local health departments have become adept at crisis management and deploying staff to meet the latest threat, said Joshua Sharfstein, former Baltimore health commissioner and Maryland secretary of health.
So the public may not see the effect of the budget cuts when a crisis strikes. But public health officials do.
“We found responding to Ebola [in 2014] really taxed our ability to respond to other outbreaks because we needed to pull all the staff” from other tasks, said Sharfstein, now an associate dean at the Johns Hopkins Bloomberg School of Public Health.
The same thing is starting to happen now across the country, Blumenstock said.
“State and local departments today are looking at their staff and deploying them to deal with Zika,” he said. “But if you send an epidemiologist to deal with Zika full time, that’s eight hours a day less that he’s doing foodborne surveillance or HIV surveillance or flu surveillance.”
The cuts result in other problems, often hidden from the public eye. They deprive health departments of needed expertise and trained personnel, which is difficult to replenish in a crisis. The networks of relationships that health departments have with other agencies, hospitals and doctors are often neglected and must be rebuilt every time there is an emergency. All that can lead to slow response times.
The biggest fear remains that two or more dangerous and quickly spreading diseases break out simultaneously.
“We’ve been lucky so far, and you don’t want to hope for a different scenario so you can prove your point,” Blumenstock said. “But there are tipping points, and there were times when we were close to those tipping points.”
Learn More
- A state by state look at public health funding
- Outbreaks 2015: Protecting Americans from infectious diseases
- The changing public health landscape
- Zika virus disease in the U.S.
- Assessing state, local mosquito surveillance
- Infectious disease infrastructure
This story is provided courtesy of N.C. Health News, a website covering health and environmental news in North Carolina. Coastal Review Online is partnering with N.C. Health News to provide readers with more environmental and lifestyle stories of interest about our coast. You can read other stories about health care here.



